Radiological Findings in a case of Advance staged Mesothelioma
From Department of Internal Medicine, Jersey City Medical Center/Mount Sinai School of Medicine, New Jersey, NJ-07302.

|
Image of the Issue
Radiological Findings in a case of Advance staged Mesothelioma
From Department of Internal Medicine, Jersey City Medical Center/Mount Sinai School of Medicine, New Jersey, NJ-07302.
|
|
Abstract
Chest X Ray is the initial screening test for the mesothelioma like all other the chest diseases. But computed tomography (CT) is the imaging technique of choice for charactering pleural masses. CT also gives important information regarding invasion of the chest wall and surrounding structures. Certain CT features help differentiate benign from malignant processes. This short article highlights the salient CT appearance of mesothelioma; the most common pleural tumor.
Key words
Advance staged Mesothelioma; Radiological FindingsJ Thorac Dis 2009;1:46-47. DOI: 10.3978/j.issn.2072-1439.2009.12.01.009
|
|
Mesothelioma is a malignant neoplasm originating from the
mesothelium, a protective lining that covers most of the body's internal organs. Its most common site is the pleura but it may arise
from the peritoneum and the pericardium.
Asbestos exposure is thought to be the single most important
factor in the development of mesothelioma. The clinical latency
period between asbestos exposure and mesothelioma development
is 35-40 years.
Pathological types of Mesothelioma:

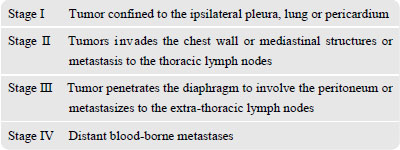
Staging of Mesotheliomas:
The two important systems for the mesothelioma classification are Burchart system and TNM classification.
The Butchart staging system [1] for malignant pleural mesothelioma is as follows
 |
|
Radiological findings of Mesothelioma
Chest X Ray:
Here we present CXR from 64 year old Hispanic male who was diagnosed with advanced mesothelioma;
The most common mesothelioma finding on radiographs is unilateral, concentric, plaque like, or nodular pleural thickening.Pleural effusions are common and may obscure the presence of the
un derlying pleural thickening. The tumor frequently extends into
the fissures, which become thickened and irregular in contour. A
slight right-sided predominance is observed, possibly because of a
larger pleural surface area. The tumor can rigidly encase the lung,
causing compression of lung parenchyma, diaphragm elevation, inter-costal space narrowing, and mediastinal shift toward the tumor.
Calcified pleural plaques are present in 20% of patients with
mesothelioma and are usually related to the previous asbestos exposure.
Lung nodules and hilar masses usually result from direct
mesothelioma tumor extension into the lung parenchyma and mediastinal structures, such as lymph nodes, the pericardium, and the
heart. Although usually unilateral, direct extension of the tumor
across the mediastinum into the contralateral hemi-thorax does occur.
Although a definite diagnosis cannot be made on the basis of
plain film findings, new unilateral pleural thickening or effusion in
a patient who has a history of exposure to asbestos is highly suggestive of mesothelioma.

Figure.1
Chest X-ray showing a large mass on left side with the slight shift of mediastium towards right.
|
|
Computed Tomography
Here we show the CT scan of the chest from the same patient diagnosed with advanced mesothelioma;
CT scan findings are similar to those of plain films but are seen
better and in more detail. Furthermore, pleural thickening and effusion can be distinguished with CT scanning.
Nodular pleural thickening, pleural thickening greater than 1 cm, involvement of the
mediastinal pleural surface, and concentric pleural thickening are
all highly suggestive of malignant pleural disease, either mesothelioma or metastases. The tumor extent along the pleural surfaces
and into the mediastinum, diaphragm, or chest wall can be evaluated much better with CT scanning than plain radiography. Chest
wall invasion manifests as obliteration of fat planes or chest wall
nodules. Diaphragmatic invasion, ascites, and omental caking are
common CT scan findings of peritoneal mesothelioma.
Benign pleural plaques or pleural thickening from asbestos exposure may mimic the appearance of nodular pleural thickening in
patients with mesothelioma.
|
|
Conclusion
Chest radiograph is the initial screening examination but chest
radiograph has limited usefulness. The X-ray findings of mesothe
li oma are non specific and observed in other disease, including
metastatic carcinoma, lymphoma and benign asbestos disease. Disease extent is frequently underestimated in radiographs. CT scanning provides more and better information than plain radiography
with regard to tumor characteristic and extent. But neither CT scan
nor MRI provides unequivocal diagnosis of mesothelioma and tissue biopsy is always required for the definitive diagnosis.

Figure.2
This CT scan is showing:
1. Large soft tissue mass lesion in the left chest cavity.
2. Narrowing of the left upper lobe pulmonary artery which is incased
by the soft tissue mass lesion.
3. Mild narrowing of the left lower lobe pulmonary artery is also present.
|
|
References
Cite this article as: Aziz F. Radiological Findings in a case of Advance staged Mesothelioma. J Thorac Dis 2009;1:46-47. doi: 10.3978/j.issn.2072-1439.2009.12.01.009
|

