Treatment of advanced non small cell lung cancer
Division of Medical Oncology, "S.G. Moscati" Hospital, Avellino, Italy

|
Review Article
Treatment of advanced non small cell lung cancer
Division of Medical Oncology, "S.G. Moscati" Hospital, Avellino, Italy
|
|
Abstract
Lung cancer is the major cause of cancer death in the world. Non Small Cell Lung Cancer (NSCLC) accounts approximately 80-85% of all lung cancer diagnosis; the majority of patients will be diagnosed with non operable, advanced-stage disease. Palliative chemotherapy and/or radiotherapy represent the standard of care of this disease. Platinum based doublets with third generation agents are considered the standard of first line advanced NSCLC treatment. However, data arising from the availability of pemetrexed suggest that histology could play a key role in decision making. Advances in understanding of the molecular pathogenesis of lung cancer have led to the identification of several specific targets such as vascular endothelial growth factor (VEGF) and epidermal growth factor receptor (EGFR) for therapeutic agents. Bevacizumab is the first recombinant humanized monoclonal antibody (mAb) binding VEGF to demonstrate clinical benefit and a rather survival prolongation in combination with chemotherapy in the treatment of non squamous chemo-naive advanced NSCLC patients. Two types of anti-EGFR targeting agents have reached advanced clinical development: mAbs and small molecule inhibitors of the EGFR tyrosine kinase enzymatic activity (TKIs). Among TKIs gefitinib has been tested in several phase II-III studies showing an improvement in survival and responses in first, second and third line treatment in selected patients with specific clinical and molecular characteristics. Furthermore, erlotinib has showed to significantly improve survival in an unselected population of patients following the failure of one or two chemotherapy regimens. This review will discuss the different therapeutic options for first and second line treatment in the clinical practice.
Key words
non small cell lung cancer; pemetrexed; bevacizumab; erlotinib; gefitinib
J Thorac Dis 2011;3:122-133. DOI: 10.3978/j.issn.2072-1439.2010.12.08
|
|
Introduction
Non-small cell lung cancer (NSCLC) is the leading cause of cancer-related death in the world. NSCLC is a heterogeneous aggregate of histologies, including squamous cell carcinoma, adenocarcinoma and large cell carcinoma, its represents approximately 80% to 85% of all lung cancers (1). While public awareness of this cancer and its associated early warning signs has improved along with the increasing use of screening techniques, the majority of patients will have advanced-stage non operable disease at the time of diagnosis.
The aim of treatment, in this setting of disease, is to slow down the progression of the disease, to relieve the patients from the lung cancer symptoms and, whenever possible, to increase the overall survival (OS). In first line treatment doublets containing platinum compounds represent the standard of care in advanced NSCLC, reporting a response rate (RR) racing from 20% to 35% with a median survival time (MST) of about 10 months (2). However, most patients receiving front-line chemotherapy experience disease progression. The availability of several new active drugs in second-line treatment suggests that this strategy can now be considered a standard of care for patients with a good performance status (PS) who progressed to first-line treatment. The chemotherapeutic agents docetaxel and pemetrexed and the biologic agent erlotinib are now available in clinical practice. The major progresses in the understanding cancer biology and mechanism of oncogenesis have allowed to identify several potential molecular targets for cancer treatment such as vascular endotelial growth factor (VEGF) and its receptors (VEGFRs) and epidermal growth factor receptor (EGFR).
Bevacizumab, an anti-VEGF recombinant humanized mAb, and the EGFR small molecules inhibitors such as gefitinib and erlotinib are now available in clinical practice in first or second-line treatment.
This review will discuss the current status of first and second line treatment in the management of advanced NSCLC patients.
|
|
First line treatment of advanced NSCLC
The role of chemotherapy in clinical practice
Since 1990s, it was demonstrated that for suitable patients (good
PS), cisplatin-based chemotherapy is associated with a small
survival advantage over best supportive care (BSC) in metastatic
NSCLC. The available in the past decade of newer cytotoxic
agents with activity in the management of NSCLC led to the
development of a large number of clinical trials testing these
agents either alone or in combination with platinium based
chemotherapy. The results of four large multicenter randomized
clinical trials evaluating these agents in combination with either
cisplatin or carboplatin have been reported over the past few
years and have yielded similar results (3-6). It is clear from
these studies that no single regimen demonstrated a significant
superiority over any other combination. In these studies median
OS was approximately 8-10 months. However, in the last three
years important advances have been achieved in the treatment of
advanced NSCLC (7).
Histology of NSCLC has never been essential in the choice
of first-line treatment; however, recent evidences arising from
the availability of pemetrexed show that histology represents an
important variable in decision making (8).
Pemetrexed is a novel multi-targeted antifolate chemotherapy
agent; its primary mechanism of action is to inhibit at least three
different enzymes in the folate pathway: thymidylate synthase
(TS), dihydrofolate reductase (DHFR), and glycinamide
ribonucleotide formyl transferase (GARFT) (9).
In vitro studies indicated that tumour cell lines expressing
high levels of TS or DHFR have reduced sensitivity to
pemetrexed, suggesting that increased expression levels might
correlate with reduced clinical efficacy (10).
A large non-inferiority phase III trial randomized
chemotherapy-naive advanced NSCLC patients to receive
either cisplatin plus gemcitabine or cisplatin at the same dose
plus pemetrexed for a maximum of six cycles. OS, the primary
end-point of this study, was 10.3 months in both arms (HR
0.94; 95% CI, 0.84 to 1.05) and survival rates at 1-year were
43.5% and 41.9% for cisplatin/pemetrexed and cisplatin/
gemcitabine, respectively. Progression free survival (PFS) was
also non-inferior (4.8 vs 5.1 months, respectively; HR 1.04) and
RR was 30.6% in the cisplatin/pemetrexed arm compared to
28.2% in cisplatin/gemcitabine arm. For cisplatin/pemetrexed
combination treatment, the rates of grade 3/4 neutropenia,
anaemia, and thrombocytopenia (P<0.001); febrile neutropenia
(P=0.002); and alopecia (P<0.001) were significantly lower,
whereas grade 3/4 nausea (P=0.004) was more common(11).
A pre-planned analysis of this trial for histology subtype of
NSCLC, reported that non-squamous patients had a longer
MST on cisplatin/pemetrexed (11 months) than on cisplatin/
gemcitabine (10.1 months; HR 0.84, P=0.011); adenocarcinoma
12.6 vs 10.9 months, respectively (HR 0.84, P=0.03); largecell
carcinoma: 10.4 vs 6.7 months, respectively (HR 0.67,
P=0.03). Whereas squamous patients had a MST of 10.8
months on cisplatin/gemcitabin compared to 9.8 with cisplatin/
gemcitabine (HR 1.23, P=0.05). The OS for patients with a
generic diagnosis of NSCLC not otherwise specified (NOS),
did not show a significant difference in survival between the
two treatment arms. Similarly, non-squamous patients showed a
trend that was not statistically significant for a longer PFS time
on cisplatin/pemetrexed than on cisplatin/gemcitabine (5.26
and 4.96 months, respectively HR 0.95, P=0.349). Squamous
patients had a shorter PFS time on cisplatin/ pemetrexed than
on cisplatin/gemcitabine (4.4 and 5.5 months, respectively; HR
1.36, P=0.002). RR were higher in the cisplatin/pemetrexed
arm compared to cisplatin/gemcitabine arm in patients with
adenocarcinoma (28.9% vs 21.7%) or other NSCLC histotypes
(28.3% vs 21.2%); a higher RR occurred in patients with
squamous cell carcinoma (23.4% vs 31.4%) on cisplatin/
gemcitabine. For patients with large cell carcinoma, RR was
not statistically different between the two treatment arms
(12). These results may be due to a higher expression of TS in
squamous cell carcinoma and lower in adenocarcinomas, leading
to lower sensitivity to pemetrexed in the squamous and higher in
adenocarcinoma histotype.
Based on these data pemetrexed in combination with cisplatin
has been granted as first-line treatment of patients with advanced
NSCLC other than predominantly squamous cell histology.
Another smaller phase III trial comparing carboplatin plus
pemetrexed or gemcitabine showed no significant difference in
the primary end point (health-related quality of life) of this study.
A higher rate of grade 3/4 hematologic toxicity was reported in
patients who received gemcitabine/carboplatin compared to
which treated with pemetrexed/carboplatin: leucopoenia (46%
vs 23%, P<0.001), neutropenia (51% vs 40%, P=0.024), and
thrombocytopenia (56% vs 24%, P<0.001). No difference in
OS between the two treatment arms was reported (7.3 months
in pemetrexed/carboplatin arm vs 7.0 months in gemcitabine/
carboplatin arm; P=0.63). Multivariate analyses and interaction
tests did not demonstrate any significant associations between
histology and survival (13) (Table 1).

The role of anti-angiogenic agents in clinical practice
Advances in understanding of the molecular pathogenesis of
lung cancer have led to the identification of several specific
targets for therapeutic agents. Angiogenesis is known to be
essential for the development and progression of cancer.
VEGF is a critical mediator in tumor angiogenesis for many solid malignancies, including NSCLC cancer. Inhibition of
tumor-related angiogenesis has become an attractive target for
anticancer therapy.
Bevacizumab
Bevacizumab is a humanized mAb directed against the VEGF;
its consists of 93% human and 7% murine components and it
recognizes all isoforms of VEGF ligands with Kd of 8 x10-10
M. Bevacizumab contains two identical light chains (214 amino
acid residues) and two heavy chains (453 residues) with a total
molecular weight of 149 kDa (14).
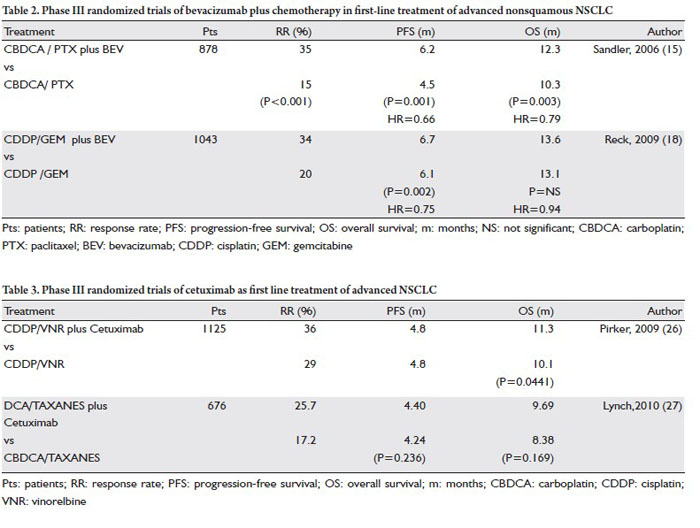
Two randomized phase III trials compared the combination
of bevacizumab with chemotherapy versus chemotherapy alone
in the treatment of advanced NSCLC.
The first multicenter phase III clinical trial (ECOG 4599)
evaluated bevacizumab plus carboplatin and paclitaxel (BCP, pts
= 434) versus carboplatin and paclitaxel alone (CP, pts = 444)
in advanced chemo-naive non squamous NSCLC patients. OS
was significantly longer in patients receiving BCP compared
to those treated with chemotherapy alone (12.3 vs 10.3
months, respectively; HR 0.80, P=0.003); PFS was 6.2 and 4.5
months (HR 0.66, P<0.001) in the two treatment arms, with a
corresponding RR of 35% and 15%, respectively (P<0.001) (15).
The addition of bevacizumab to chemotherapy resulted
globally well tolerated, but more toxic then chemotherapy alone,
the rates of clinically significant bleeding were 4.4% and 0.7%
respectively (P<0.001).
A pre-planned subgroup analysis of this trial regarding the
survival and safety outcomes based on histology has been
recently published. For adenocarcinoma histology an increased
OS has been reached for patients receiving BCP compared to
patients treated with chemotherapy alone (14.2 months vs 10.3
HR 0.69). No unexpected toxicities have been observed among
histology subtype (16).
The restriction of the patients population to non squamous
histology, based on life-threatening or fatal haemoptysis
occurring in 4 of 13 patients with squamous histology who
received a BCP regimen in a phase II study, have determined in
this trial a lower incidence of grade ≥3 pulmonary hemorrhage
(17). Regarding the squamous histology, a retrospective
analysis of the clinical and radiographic risk factors associated
with severe pulmonary hemorrhage reported only the baseline
tumor cavitation as a potential risk factor with no influence by
squamous histology and tumor central localization.
Recently, a phase II trial (BRIDGE) evaluated the safety of
adding bevacizumab to carboplatin/paclitaxel chemotherapy in
forty-seven untreated advanced squamous NSCLC patients. The
incidence of grade ≥ 3 pulmonary haemorrhage in this study was
3.2% (1 pt) and no new safety signals were identified, however
other clinical trials will performed to clarify this question (18).
Another large phase III trial (AVAIL) evaluated the
combination of bevacizumab (15 mg/kg or 7.5 mg/kg every 3
weeks until disease progression) with gemcitabine /cisplatin
versus the same chemotherapy regimen without bevacizumab
in previously untreated, advanced non-squamous NSCLC
patients. A significantly longer PFS, the primary study endpoint,
was observed in patients randomized to receive bevacizumab
therapy [6.1 months in the control arm, 6.7 (HR 0.75, P=0.002),
and 6.5 months (HR 0.82, P= 0.03) in 7.5 mg/kg, and 15 mg/
kg bevacizumab arms, respectively]; also the RR and response
duration were significantly increased in both bevacizumab
treatment arms (20%, 34%, and 30.4%, in the control, 7.5 mg/
kg, and 15 mg/kg bevacizumab arms, respectively) (19). No
difference in median OS was observed among all treatment
groups (20). It is likely that the unprecedented high use of
multiple second-line therapies in this trial is the main reason
why the PFS benefit did not translate into an OS benefit. The
ECOG 4599 and AVAIL trials represent the first evidence of
an improvement in treatment outcomes of chemotherapy with
targeted therapies in the first line treatment of advanced NSCLC
(Table 2).
Bevacizumab is currently licensed for use in combination with carboplatin plus paclitaxel for the first line therapy at dose of 15
mg/kg in patients with advanced NSCLC in United States, or in
addition to platinum based chemotherapy in Europe at dose of
7.5 mg/kg or 15 mg/kg.
A meta-analysis of four randomized phase II-III study testing
the addition of bevacizumab to different platinum-doublets
as first line treatment of NSCLC, has been recently reported.
This meta-analysis demonstrated an improvement in both OS
(HR 0.89; P=0.03) and PFS (HR 0.72; P<0.001) in patients
treated with bevacizumab plus chemotherapy. Patients with
adenocarcinoma histlogy, recurrent or IIIb stage, non white race
and body weight loss ≤5% had a significant higher OS compared
to other corresponding group of patients (21).
The results of a multicenter, single-arm study (SAIL) have
confirmed, in a real-world population, the safety and efficacy
outcomes of bevacizumab treatment just reported in pivotal
phase III trials (22).
Data emerging from several studies confirm the safety of
bevacizumab-based therapy for the treatment of NSCLC patients
with treated central brain metastases (CNS) (23,24).
However, further safety data have demonstrated that the risk
of bleeding is similar in patients with untreated brain metastases
receiving bevacizumab compared to those do not across various
tumor types.
Based on these data, the EMEA that approved the drug use
combined to any platin-based chemotherapy, removed the
controindication concerning the use of bevacizumab in untreated
CNS (25).
The role of EGFR inhibitors in clinical practice
Monoclonal antibodies: Cetuximab
Cetuximab is a chimeric human/murine IGg1 mAb that
selectively bind to the extracellular domain of EGFR on the
tumour cell, thereby inhibiting receptor-associated tyrosine
kinase activation (26,27).
A large randomized phase III trial (FLEX), tested a platinumbased
chemotherapy (cisplatin/vinorelbine) versus the same
chemotherapy regimen plus cetuximab as first line treatment in
EGFR-detectable advanced NSCLC patients.
The combination regimen has demonstrated a small but
statistically significant benefit in survival over chemotherapy
alone (11.3 vs 10.1 months, respectively; HR 0.871, P=0.0441)
in all histology subgroups of NSCLC. An higher ORR was
reported in patients receiving cetuximab (36% vs 29%, P=0.010),
without a difference in PFS (median 4.8 months in both groups,
HR 0.943). The grade 3 acne- like rash was the main cetuximab
related adverse event (AE) and it occurred in 10% of patients
enrolled in this trial.
This is the first study to demonstrate a survival benefit of
an EGFR-targeted agent in combination with platinum-based
chemotherapy in advanced first-line NSCLC irrespective of
histology (28).
Another multicenter randomized phase III clinical study
(BMS 099) compared the combination of cetuximab plus
carboplatin/ taxanes versus chemotherapy alone in advanced
NSCLC. The addition of cetuximab to chemotherapy did
not significantly improve PFS (4.40 months in cetuximab/
chemotherapy arm vs 4.24 months with chemotherapy alone;
HR 0.902, P=0.236). Median OS was 9.69 months in the
combination arm versus 8.38 months in chemotherapy group
(HR 0.890, P=0.169), however the survival benefit was similar
to that observed in FLEX trial, but no statistically significant. An
increase RR was reported in the combination arm compared to
chemotherapy alone (25.7% and 17.2%, respectively P=0.007)
(29) (Table 3).
A meta-analysis of individual patient data from four
randomized phase II-III studies evaluated the effect of adding
cetuximab to chemotherapy for the first-line treatment of
advanced NSCLC. All efficacy results including OS, PFS and
ORR were improved in cetuximab treated patients (HR 0.88
P=0.009; HR 0.90 P 0.045; P<0.001); and a favorable safety
profile for chemotherapy plus cetuximab combination was also
reported in this meta-analysis (30).
EMEA rejected the registration request for cetuximab
combined to chemotherapy but a further final decision is now
pending.
EGFR tyrosine kinase inhibitors: Gefitinib and Erlotinib
Gefitinib
Gefitinib is an orally available, reversible and selective EGFRTKI,
the first to have reached clinical trial testing.
The role of gefitinib as first line treatment in combination
with chemotherapy has been evaluated in two large randomized
phase III INTACT1 and INTACT2 trials (31,32). One
thousand hundred ninety three patients in INTACT 1 and
one thousand hundred thirty three in INTACT 2 study were
randomized to receive gefitinib (250 mg or 500 mg daily) in
combination with cytotoxic agents (cisplatin/gemcitabine) or
(carboplatin/paclitaxel), respectively. No survival advantage and
no difference in the secondary end points including RR and time
to progression (TTP) was seen with the addition of gefitinib to
chemotherapy, in either trial.
The major challenge for an optimal use of EGFR targeting
drugs is to define which patients are more likely to have a
therapeutic advantage from the treatment. Clinical data suggest
that TKIs are more active in certain NSCLC histotypes such as
in adenocarcinomas and in bronchioloalveolar carcinomas, in
women, in never smoker, in Asian ethnicity patients (33,34).
In 2004, three research groups have identified somatic gene
mutations within the kinase domain of EGFR, related to the response to EGFR TKIs (35-37). EGFR mutations were most
frequently detected in a subpopulation of NSCLC patients with
characteristics associated with a better treatment outcome:
female sex, non smokers, Asian origin, adenocarcinoma
histology. Approximately 90% of EGFR gene mutations affect
small region of the gene within the exons (18 to 24) which code
for the TK domain. The more common mutations are an in
frame deletion in exon 19 around codons 746 to 750 (45% - 50%
of all somatic EGFR mutations) and a missense mutation leading
to leucine to arginine substitution at codon 858 (L858R) in exon
21 (35- 45% of all EGFR mutations) (38).
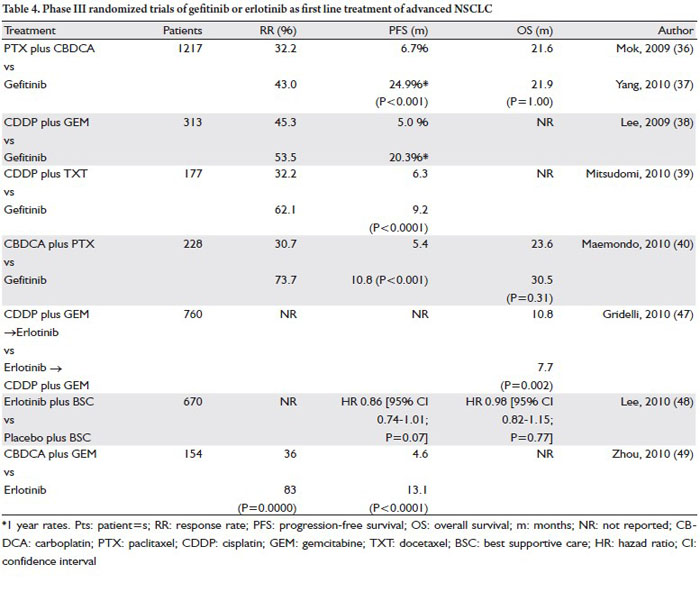
Several randomized phase III studies have compared gefitinib
to platinum-based chemotherapy in advanced NSCLC patients.
In the IPASS trial (Iressa Pan-Asia Study), advanced NSCLC
patients selected by clinical characteristics (never or light
smokers, adenocarcinoma histology) were randomly assigned to
receive gefitinib or carboplatin plus paclitaxel.
The 12-month rates of PFS were 24.9% with gefitinib and 6.7%
with carboplatin-paclitaxel (HR 0.74, P<0.0001) (39); although
OS did not differ between the two groups: 21.6 months for
who began the study on gefitinib compared to 21.9 months of
patients who had started on chemotherapy (P=1.00) (40).
In EGFR mutation positive patients (261 pts), PFS was
significantly longer in patients receiving gefitinib compared
to those treated with carboplatin-paclitaxel (HR 0.48; 95%;
P<0.001); whereas in the subgroup of EGFR wild type (176 pts),
PFS was significantly longer in patients receiving carboplatinpaclitaxel
(HR for progression or death with gefitinib, 2.85; 95%;
P<0.001).
Also the ORR was higher in patients with EGFR mutated
tumors than in those without receiving gefitinib (71.2% and
1.1%, respectively ) (39).
In the First-SIGNAL study, Korean advanced NSCLC
patients (adenocarcinoma histology and never smokers)
were randomized to gefitinib or standard chemotherapy
(gemcitabine/cisplatin) as first line treatment. OS was similar in
both groups, although PFS at 1 year was superior in the gefitinib
compared to chemotherapy group (20.3% and 5.0% respectively)
and also quality of life (QoL) is improved in gefitinib group.
Moreover a subgroup analysis showed an OS of 30.6 months in EGFR mutations positive patients and 18.4 months in those
without mutations (HR 0.845; P=0.643) treated with gefitinib
and a PFS of 8.4 and 2.1 months, respectively (HR 0.394; P=
0.0006); the ORR was also dramatically better in this subgroup
of patients (84.6% and 25.9%; respectively) (41).
In the WJTOG3405 trial, chemotherapy-naive advanced
NSCLC patients harbouring EGFR mutations were randomly
assigned to receive gefitinib or chemotherapy (cisplatin/
docetaxel). In gefitinib arm a longer PFS was reported compared
to chemotherapy group (9.2 and 6.3 months; HR 0.489, log-rank
P<0.0001, respectively); as well the RR was higher in patients
tretated with gefitinib (62.1% and 32.2%, respectively) (42).
In a more recent trial (NEJ002) gefitinib was compared to
carboplatin/paclitaxel in EGFR mutated advanced NSCLC
patients. After a planned interim analysis this trial has been
interrupted since a significantly longer median PFS (10.8 vs 5.4
months; HR, 0.30; P<0.001), as well as a higher RR (73.7% vs
30.7%, P<0.001) was reported in patients treated with gefitinib.
However the median OS was 30.5 months in the gefitinib group
and 23.6 months in the chemotherapy group (P=0.31) (43)
(Table 4).
These two phase III trials performed in EGFR mutated
patients confirm once more gefitinib to be superior to
chemotherapy in terms of PFS and RR suggesting that the EGFR
gene mutational status play an important role in the treatment
choice of advanced NSCLC.
Finally, based on these results the EMEA approved gefitinib
for the treatment of advanced NSCLC patients harbouring
EGFR mutations even in first-line setting.
Erlotinib
Erlotinib is an oral low molecular weight quinazoline-based
agent which selectively and reversibly inhibits the kinase activity
of EGFR (44).
As observed for gefitinib, the combination of erlotinib with
platinum based polichemotherapy (carboplatin/paclitaxel
and cisplatin/gemcitabine in TRIBUTE and TALENT phase
III trials, respectively) in advanced NSCLC chemo-naïve
patients, demonstrated to confer no survival advantage over
chemotherapy alone (45,46).
Several phase II trials tested erlotinib as monotherapy in
unselected chemo-naive advanced NSCLC patients showing
interesting results (47-49).
A large randomized phase III trial (TORCH) compared
erlotinib followed by chemotherapy (cisplatin/gemcitabine)
versus the same chemotherapy regimen followed by erlotinib in
advanced NSCLC unselected patients (standard Arm). This trial
was early stopped based on planned interim analysis showing an
HR of 1.40 for death in experimental arm P=0.002 and a median
OS of 7.7 vs 10.8 months in the standard arm (50).
In another phase III trial chemo-naïve advanced NSCLC
patients (ECOG PS 2/3 or PS 0/1 unfit for platinum
chemotherapy) were randomized to erlotinib plus BSC or
placebo plus BSC. Erlotinib did not improve OS (HR 0.98;
P=0.77). Pre-specified subgroup analyses showed significant
longer OS and PFS for females (HR 0.75; P = 0.04 and HR 0.64,
P< 0.001; respectively) and a clear effect on PFS was also seen
for adenocarcinoma histology (HR 0.74; P= 0.03) (51).
The important role of EGFR activating mutations suggests
the relevance of patient selection to identify which could gain
interesting clinical benefit by erlotinib as front-line therapy.
In a recent phase III trial (OPTIMAL) EGFR mutated Asian
NSCLC patients were randomly assigned to receive erlotinib
or “doublet” combination chemotherapy of gemcitabine and
carboplatin. The PFS in erlotinib arm was 13.1 compared to 4.6
months in chemotherapy arm and a higher RR was also achieved
in erlotinib arm (83% vs 36% respectively). Subgroup analysis
showed a consistent benefit with erlotinib regardless of histology,
smoking history, age, sex, and disease stage.
OPTIMAL is the first prospective trial to confirm the role
of erlotinib in advanced NSCLC patients with EGFR activating
mutations (52) (Table 4).
An impor tant prospective phase III ongoing tr ial
(EURTAC) will evaluate the efficacy of erlotinib compared
with chemotherapy in advanced caucasian NSCLC patients
harbouring EGFR gene mutations. The final results of this trial
are expected next year.
|
|
Second-line treatment in advanced non small cell
lung cancer
After or during first-line treatment several NSCLC patients have
experience of disease progression with a limited life expectancy.
Numerous variables such as disease-related symptoms, residual
toxicity of previous chemotherapy, and co morbid diseases,
could compromised the QoL. Life expectancy of these patients
is largely dependent on their PS at the start of second-line
treatment.
In recent years, the efficacy of several drugs in the
second-line setting has been demonstrated and second-line
treatment can now be considered a standard of care (53). Two
chemotherapeutic agents, docetaxel and pemetrexed, and
erlotinib are currently approved for the second line treatment
of unselected NSCLC patients, while gefitinib is approved for
clinical use only in patients with EGFR mutated tumors.
Docetaxel
In a phase III trial (TAX317), docetaxel 100 mg/m2 was
compared to BSC. The protocol was amended and the dose was
reduced to 75 mg/m2 after the evidence of a significantly higher
toxic death rate in the chemotherapy arm.
A longer TTP was observed for docetaxel compared to BSC (10.6 vs 6.7 weeks, respectively; P<0.001); also OS was
significantly longer for patients receiving docetaxel (7.0 vs 4.6
months; P=0.047). Febrile neutropenia was the most common
toxicity related to docetaxel treatment observed (11 pts in
docetaxel 100 mg/m2, three of whom died, and 1 patient in
docetaxel 75 mg/m2) (54).
In another phase III study (TAX 320), patients were
randomly assigned to receive docetaxel at dose of 100 mg/m2
or 75 mg/m2 every 3 weeks, or vinorelbine or ifosfamide at the
investigator’s discretion.
Patients in docetaxel arm achieved a longer TTP (P=0.046)
and PFS at 26 weeks (P=0.005). Although no significant
difference in OS was reported between the three treatment arms,
however the 1-year survival rate was significantly higher with
docetaxel 75 mg/m2 compared to the control treatment (32% vs
19%; P=0.025).
A greater ORR has been reported in both docetaxel arms
(10.8% for docetaxel at dose of 100 mg/m2 and 6.7% at 75 mg/
m2), compared to vinorelbine or ifosfamide (0.8% P=0.001 and
P=0.036, respectively). Patients received docetaxel had more
neutropenia and febrile neutropenia compared to control arm,
but the lower dose of docetaxel was generally well tolerated (55).
Based on the results of these two phase III trials docetaxel
was the first drug to be approved for second-line treatment of
advanced NSCLC.
Considering the toxicities related to standard 3-week
schedule of docetaxel including fatigue, myelosuppression and
pain, several randomized clinical studies have been conducted
to compare the standard schedule with the weekly schedule. The
results of these trials suggest a better toxicity profile for weekly
regimen but contrasting results regarding the OS (56-60).
A meta-analysis based on individual data from patients
enrolled in five randomized trials has compared the efficacy
of the two different schedules of docetaxel for second-line
treatment of NSCLC. No survival difference between the two
schedules, with a HR estimate of only 1.09, has been observed. This analysis confirms a significantly different toxicity profile
between the two schedules of docetaxel as febrile neutropenia
that is significantly lower with weekly schedule.
In conclusion, weekly docetaxel may be a valid alternative
to standard 3-weekly schedule for all NSCLC patients who are
candidates for a second-line chemotherapy (61).
Pemetrexed
In a phase III trial advanced NSCLC patients after failure of
one prior chemotherapy regimen, were randomly assigned
to receive pemetrexed or docetaxel. The ORR was 9.1% and
8.8%, the MST 8.3 vs 7.9 months (P = not significant) for
pemetrexed and docetaxel, respectively. A median PFS of 2.9
months and the 1-year survival rate of 29.7% were reported in
each arm. Pemetrexed produced similar results and was better
tollerated than docetaxel, in-fact an higher incidence of grade 3-4
neutropenia, neutropenic fever and neuropathy was reported in
docetaxel arm (62).
A retrospective analysis of this trial showed no significant
difference in outcome or toxicity between elderly and younger
patients (63). Elderly patients receiving pemetrexed or docetaxel
had a MST of 9.5 and 7.7 months compared to 7.8 and 8.0
months for younger patients treated with pemetrexed or
docetaxel respectively. Elderly patients treated with pemetrexed
had a longer TTP and OS than their counterpart patients
treated with docetaxel (not statistically significant). Pemetrexed
demonstrates a more favorable toxicity profile than docetaxel:
febrile neutropenia was less frequent in elderly patients treated
with pemetrexed (2.5%) compared to those receiving docetaxel
(19%; P=0.025).
A different activity of pemetrexed in different histotypes of
NSCLC has been also confirmed in the second-line treatment
by a retrospective analysis of this trial. A longer OS was observed
in non-squamous patients receiving pemetrexed than docetaxel
(9.3 vs 8.0 months; HR 0.78; P=0.047), conversely squamous
patients had a shorter OS with pemetrexed treatment compared
to docetaxel (6.2 vs 7.4 months; HR 1.56; P= 0.018). Nonsquamous
patients had a little longer PFS with pemetrexed
than docetaxel (3.1 vs 3.0 months; HR 0.82; P=0.076), while
squamous patients achieved a little shorter PFS on pemetrexed
than docetaxel (2.3 vs 2.7 months, respectively; HR 1.40;
P=0.046). Differences in RR according to histology were also
observed; in fact a higher RR was reported in adenocarcinoma or
large cell carcinoma patients receiving pemetrexed compared to
those treated with docetaxel; whereas in patients with squamous
or other NSCLC histology RR favoured docetaxel (64).
A phase III study compared high dose (900 mg/m2) to
standard dose of pemetrexed in advanced NSCLC patients
after failure of one platinum based chemotherapy regimen.
No statistical difference was reported between two treatment
groups for MST (6.7 vs 6.9 months, HR 1.0132), PFS (2.6 vs 2.8 months, HR 0.9681) or best ORR (7.1% vs 4.3%; P=0.16);
however the incidence of toxicities were higher in experimental
arm (65).
Erlotinib
In a phase III, placebo-controlled trial (BR21) erlotinib was
compared to BSC in pre-treated advanced NSCLC patients
who have received one or two regimens of combination
chemotherapy and not be eligible for further chemotherapy.
The RR was 8.9% in the erlotinib arm and less than 1% in the
placebo group (P<0.001); a PFS of 2.2 and 1.8 months was
reported, respectively (P<0.001; HR 0.70). A significant survival
advantage of 2 months was observed in all patients subgroup
treated with erlotinib compared to placebo (P<0.001; HR 0.7)
(66).
An analysis of this trial showed that smoking status may be
the most important predictor of a survival benefit with erlotinib
treatment in fact never smokers treated with erlotinib had a
significantly higher survival rate than patients receiving placebo
(HR 0.4; P=0.01) (67).
A QoL analysis has demonstrated a significant benefit
of erlotinib in improving not only survival but also time to
deterioration for all three major symptoms related to the disease
(cough, dyspnoea and pain) (68). Based on these results,
erlotinib has been approved by the FDA and EMEA in October
2005 for the treatment of chemotherapy-resistant advanced
NSCLC patients and is actually approved worldwide for second
and third-line treatment of unselected advanced NSCLC
patients.
The large, global, open-labeled, phase IV trial TRUST study
included more than 6,500 patients evaluated safety and efficacy
of erlotinib in patients with advanced stage IIIB/IV NSCLC who
had previously failed on or were considered unsuitable to receive
standard chemotherapy or radiotherapy and were ineligible for
other erlotinib trials. In patients with advanced NSCLC, the
PFS and OS in this study were 3.25 months and 7.9 months,
respectively, and the disease control rate was 69% .Results from
the TRUST study suggest that erlotinib can benefit a wide range
of patients, including those who have previously been thought
unlikely to benefit from this treatment (69).
Gefitinib
A large multicenter, randomized phase III trial (INTEREST),
has compared gefitinib versus docetaxel in previuosly treated
advanced NSCLC patients.
The results overall were very similar for the two treatments:
MST for docetaxel-treated patients was 8.0 months compared
to 7.6 months for patients receiving gefitinib (HR 1.020); 1-year
survival rate was 34% and 32%, respectively. The RR was slightly
higher with gefitinib, 9.1% vs 7.6%.
The superiority of gefitinib in patients with high EGFR-gene-copy number (co-primary endpoint) was not met (72 vs 71 events; HR 1.09, P=0.62; MST 8.4 vs 7.5 months).
In the gefitinib group, the most common AE were rash or acne
and diarrhoea whereas in the, neutropenia, asthenic disorders
and alopecia were most frequently reported in docetaxel group
(70).
Molecular analysis of biomarkers including EGFR copy
number by fluorescent in situ hybridization (FISH), EGFR
protein expression by immunohistochemistry (IHC), EGFR and
KRAS mutations showed that survival was similar for gefitinib
and docetaxel, with no statistically significant difference between
treatments and no significant treatment by biomarker status
interaction tests. However among EGFR mutated patients, PFS
advantage in favour of gefitinib was reported (PFS; HR 0.16;
P=0.001) and also a higher ORR was also observed (42.1% and
21.1%, respectively; P=0.04) (71).
In a phase III trial (V-15-32), pre-treated Japanese advanced
NSCLC patients were randomized to receive gefitinib or
docetaxel. Non-inferiority in OS was not achieved (HR
1.12) according to predefined criteria (upper CI limit for HR
<1.25); however, no significant difference in OS (P= 0.330)
or PFS (P=0.335) was evident between treatments. Gefitinib
significantly improved RR, TTP and QoL compared to docetaxel.
However, in this study cross-over of treatments was allowed,
which would have possibly affected the survival results (72).
In a randomized phase III trial (ISTANA) has been compared
gefitinib to docetaxel in pretreated Asian NSCLC patients. This
study showed a longer PSF (HR 0.73), and an improvement in
RR (28.1% vs 7.6%, P=0.0007) in favour to gefitinib (73).
In both trials, gefitinib provided RR around 25% and median
PFS around 2 to 3 months representing in unselected East Asian
patients the general treatment outcomes.
Gefitinib use is not actually approved by regulatory agencies
in the second line treatment of unselected NSCLC patients.
|
|
Conclusion
In the last few years, relevant advances have been reached in
advanced NSCLC treatment. Platinum-based chemotherapy is
the standard of treatment for the majority of patients, however
new chemotherapy drugs and targeted agents have expanded
treatment options for this disease. Recent evidences suggest that
histology represents an important variable in decision making.
In fact, in first line treatment of non-squamous NSCLC patients,
bevacizumab and pemetrexed have improved outcomes and
modified treatment algorithms, while fewer therapeutic options
are actually available for squamous histology patients which
could be treated with chemotherapy containing platinum plus a
third generation cytotoxic agent.
The identification of several factors, including both the
genetic profile of the patients and the biological characteristics of
the disease could guide the clinician’s choice.
Considering the excellent benefit and better safety profile of
gefitinib in patients with tumours harboring EGFR-mutations,
it could represents the standard in first- line treatment for this
subgroup of patients while erlotinib is waiting for the regulatory
agencies approval.
Several agents are actually approved for the second line
treatment, the choice of second line treatment is based on
histological and biological characteristics of the tumor, PS of
patients and on the drugs already used in first line.
In addition, novel cytotoxic agents are in clinical development
including new platinum analogs such as picoplatin (a cisplatin
analog), ABT-751 (a sulfonamide) and tubulin binding agents
(TBAs) such as the epothilones. New targeted agents and their
combinations with chemotherapy agents are also being explored
in clinical research in hopes to improve treatment options for
advanced NSCLC patients. Future challenges involve identifying
predictors of response and efficacy for targeted therapies and
selecting the optimal therapy for maximum survival benefit in.
|
|
References
Cite this article as: Bareschino MA, Schettino C, Rossi A, Maione P, Sacco PC, Zeppa R, Gridelli C. Treatment of advanced non small cell lung cancer. J Thorac Dis 2011;3(2):122-133. doi: 10.3978/j.issn.2072-1439.2010.12.08
|

