Case series of treatment approaches in fit nonagenarians with stage IV non-small-cell lung cancer
Division of Hematology/Oncology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA

|
Case Report
Case series of treatment approaches in fit nonagenarians with stage IV non-small-cell lung cancer
Division of Hematology/Oncology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA
|
|
Abstract
An increasing number of nonagenarians are treated for non-small-cell lung cancer (NSCLC); however guidelines and case series describing the care of very elderly patients with advanced NSCLC are not available.Medical records of patients treated at Beth Israel Deaconess Medical Center between 2007 and 2009 who had NSCLC were reviewed, and those with stage IV NSCLC and age 90 or older were included in this case series.Three successive fit nonagenarians were identified out of the one hundred and one cases with stage IV NSCLC, and their clinical course was summarized. The first case depicts a conservative approach (best supportive care), while the later cases describe the use of platinum-based (carboplatin-pemetrexed) and anti-epidermal growth factor targeted therapies. This series illustrates the diversity of approaches now available and the evolving treatment paradigm as it applies to fit elderly with NSCLC, including nonagenarians. It also emphasizes the importance of considering performance status rather than biologic age when making treatment decisions.
Key words
nonagenarian; mutation; lung cancer; non-small-cell lung cancer; metastasis; EGFR; EGFR inhibitor
J Thorac Dis 2011;3:141-143. DOI: 10.3978/j.issn.2072-1439.2011.03.02
|
|
Introduction
Lung cancer contributes to the greatest number of cancer-related deaths globally. Within the United States, the average age of diagnosis is greater than 70 years of age and the prevalence among the very elderly is increasing (1). Patients at these age extremes present treatment dilemmas for oncologists.
Here we describe a single center’s experience treating three successive fit patients > 90 years of age with stage IV non-small-cell lung cancer (NSCLC).
|
|
Materials and methods
We reviewed all records of NSCLC patients seen in the thoracic oncology outpatient clinic at BIDMC between 2007 and 2009 for whom care was provided by a dedicated medical thoracic oncologist. Patients with ≥ 90 years of age and stage IV NSCLC were included.
The following variables were recorded: date of diagnosis, date of death, patient’s demographics information (sex, ethnicity, patient’s smoking status and pack-years), patient’s Eastern Cooperative Oncology Group (ECOG) performance status (PS), tumor histology, Charlson Co-morbidity Index (CCI) (2), and treatment received. Descriptive case reports were summarized for each identified nonagenarian.
We obtained approval from the Beth Israel Deaconess Medical Center (BIDMC)’s Institutional Review Board (IRB) for access to the online medical records of cases with a diagnosis of NSCLC seen at BIDMC.
|
|
Statistics/endpoints
Survival, time to progression and sites of progression were assessed. Survival was defined as time from onset of treatment to death. Time to progression was defined as time from onset of treatment to first event, including failure at any site, local or distant or death. Survival data were calculated using the Kaplan-Meier product limit method. Survival estimates were obtained using SAS version 9.3.
|
|
Results
Identification of patients
We identified 101 patients with advanced stage IV NSCLC who had their longitudinal care provided primarily by a dedicated medical thoracic oncologist at BIDMC. Of these, 3 patients (3/101, 2.97%) fit our age criteria of being nonagenarians at time of diagnosis.
Description of cases
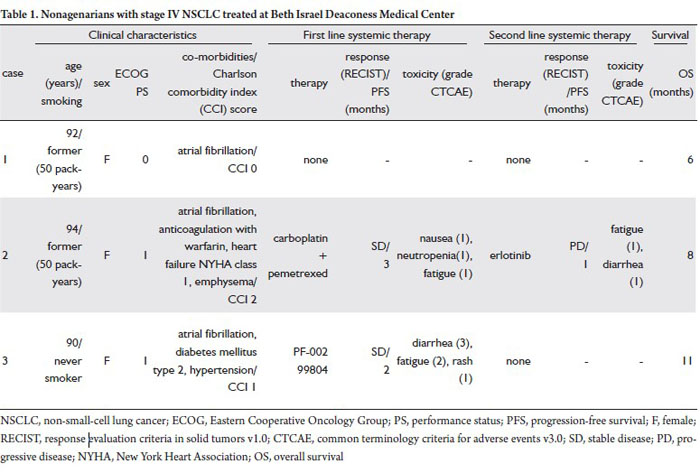
Case 1
A 92 year-old Caucasian woman, former smoker (50 pack-years), presented with pleuritic chest pain, hemoptysis and weight loss. Computed tomography (CT) of chest displayed a 3cm left lowerlobe lung mass. Fine needle aspiration (FNA) of the lesion
revealed NSCLC not otherwise specified (NOS). Positron
emission tomography (PET)/CT confirmed the presence of the
left lower lobe mass, a single hepatic lesion and metastasis within
the right femoral neck. Magnetic resonance imaging (MRI)
of the brain did not show metastasis. The patient’s ECOG PS
was 0, and her CCI score prior to the diagnosis of cancer was 0.
Systemic chemotherapy in the form of single agent vinorelbine
was offered. However, the patient opted to forgo chemotherapy
in favor of best supportive measures (Table 1). She subsequently
developed recurrent hemoptysis and right hip pain for which she
received palliative radiation to lung and bone with symptomatic
relief. She was transitioned to hospice care. Her survival was 6
months.
Case 2
A 94 year-old Caucasian woman, former smoker (50 packyears), presented with progressive dyspnea and cough. CT of chest revealed a 5cm right lower lobe mass with multiple bilateral pulmonary nodules. FNA of the dominant mass revealed NSCLC NOS. MRI of the brain was free of metastasis. The patient had an ECOG PS of 1, a CCI score of 2 prior to being diagnosed with NSCLC and was interested in pursuing chemotherapy. She received 1 cycle of carboplatin (AUC 2) and pemetrexed (500 mg/m2). Two weeks later, she developed dyspnea related to heart failure requiring hospitalization. Once improved, she resumed chemotherapy with pemetrexed alone for an additional 3 cycles with stable disease as her best response (Table 1). Treatment related toxicities were mild (Table 1). She then was found to have progression of her disease with malignant airway obstruction requiring stenting of the bronchus intermedius and a right-sided pleural effusion. Second line systemic therapy consisted of a course of single agent erlotinib (administered at 100 mg oral every other day) with limited toxicity (Table 1), however the patient progressed further and entered hospice care. Her survival was 8 months.
Case 3
A 90 year-old East Asian woman, and never smoker, presented
with chronic cough, hoarseness, left recurrent laryngeal nerve
paralysis and dysphonia. CT of chest and neck revealed a 2.4cm
mass in the left upper mediastinum, a 1.6cm nodule in the right
lower lobe, supraclavicular lymphadenopathy and a moderate
right-sided pleural effusion. FNA of the left upper paratracheal
lesion revealed poorly-differentiated adenocarcinoma. Analysis
for an epidermal growth factor receptor (EGFR) mutation was
inconclusive due to insufficient tissue for DNA extraction from
the FNA cell block. MRI of the brain revealed no metastasis.
The patient’s ECOG PS was 1 and CCI score of 1 prior to
diagnosis of NSCLC. She was not interested in pursuing
conventional chemotherapy. Given the increased likelihood thather tumor carried an EGFR mutation, she was offered enrollment
in a clinical trial of a novel oral EGFR tyrosine kinase inhibitor
(PF-00299804, NCT00818441). She tolerated 2 cycles of
treatment [complicated by diarrhea, fatigue, and rash (Table 1)]
with stable disease as best response before experiencing clinical
progression with recurrent right pleural effusion requiring an
indwelling pleural drainage catheter. She was transitioned to
home hospice. Her survival was 11 months (Table 1).
|
|
Discussion
NSCLC remains the predominant subtype of primary lung
malignancies. While improved survival among patients with
advanced NSCLC has been demonstrated with platinumdoublet
chemotherapy (with or without bevacizumab), it
remains modest and seldom exceeds 12 months (3). Patients
with NSCLC carrying EGFR mutations (more often never or
light smokers with adenocarcinoma of the lung) and treated with
gefitinib experience superior progression-free survival when
compared to a platinum-doublet (4). EGFR tyrosine kinase
inhibitors have increasingly become an option for first-line
therapy in select patients with activating EGFR mutations (4).
Perhaps due to the limited and previously unknown survival
benefit from conventional chemotherapies and out of concern
for tolerability, the majority of elderly patients have historically
not received systemic therapy for advanced NSCLC (1).
Support for the use of chemotherapy in patients over 70 years
of age with stage IV NSCLC evolved when phase II and III
studies demonstrated the activity of third-generation therapies
vinorelbine, gemcitabine, paclitaxel and docetaxel as single
agents (5). At the time, this led to the incorporation of singleagent
chemotherapy into some practice guidelines, particularly
for the elderly (1,3). However, more recently, the 2009 American
Society of Clinical Oncology Clinical Practice Guideline Update
on Chemotherapy for Stage IV NSCLC recommends that age by
itself should not preclude the choice of doublet chemotherapy in
the elderly (3). This recommendation is now further supported
by recent data showing improved response, progression-free and
overall survival in patients age 70-89 with NSCLC who received
platinum-doublet therapy, with carboplatin and paclitaxel, in
comparison to single agent therapy in the form of gemcitabine
or vinorelbine followed by second line therapy with erlotinib
in both arms (median survival: 10.4 months vs 6.2 months;
HR = 0.60; P=0.0001) (6). For the fit elderly with NSCLC, a
platinum-doublet may be the new standard of care.
However, evidence-based data to guide therapy of the very
elderly (≥ 90 years) with NSCLC are lacking. Our series shows
the diversity of approaches used at one center over the course
of three successive fit patients ≥ 90 years of age at the time of
diagnosis. Case 1 reveals a more conservative approach, where
single agent vinorelbine was offered as first-line, reflecting the standard of care at the time, but the patient ultimately declined
chemotherapy. The patient’s survival of 6 months was consistent
with expected survivals of best supportive care (1,3). Cases 2
and 3 reflect more of the current standards with regard to using
first-line platinum-doublet and anti-EGFR targeted therapy,
respectively (2,4,6). Both patients had an ECOG PS 1, lacked
significant co-morbidities (based on CCI scores less than or
equal to 2) and experienced survivals in excess of 6 months
(Table 1). Such examples illustrate the importance of evaluating
functional status rather than biologic age when making
treatment decisions, as supported by current practice guidelines
from the American Society of Clinical Oncology (3). Indeed, a
recent series of cancer cases of mostly fit nonagenarians treated
between 1993 and 2006 (10 of the 177 patients had lung cancer)
demonstrated low treatment-related mortality and acceptable
outcomes in patients receiving standard stage-specific therapies
(7).
Treatment plans for stage IV NSCLC must be tailored to each individual patient with particular attention paid to performance status and goals of care, even for nonagenarians. This area deserves further study through the inclusion of fit nonagenarians with stage IV NSCLC in prospective clinical trials.
|
|
References
Cite this article as: Britt GJ, Gaughan EM, Nguyen KSH, Warner JL, Goldstein MA, Huberman MS, Costa DB. Case series of treatment approaches in fit nonagenarians with stage IV non-small-cell lung cancer. J Thorac Dis 2011;3(2):141-143. doi: 10.3978/j.issn.2072-1439.2011.03.02
|

