Thoracic malignant solitary fibrous tumors: A population-based study of survival
Department of Radiation Oncology, University of Rochester Medical Center, Rochester, NY 14642, USA

|
Original Article
Thoracic malignant solitary fibrous tumors: A population-based study of survival
Department of Radiation Oncology, University of Rochester Medical Center, Rochester, NY 14642, USA
|
|
Abstract
Introduction: This study characterizes the overall survival (OS) and cause specific survival (CSS) of patients with thoracic malignant solitary fibrous tumors.
Methods: Eighty-two patients with malignant solitary fibrous tumors of the lung, pleura or mediastinum, diagnosed from 2001-2007, were retrospectively analyzed using the population-based Surveillance, Epidemiology, and End Results database.
Results: Among 77 patients with available staging information, 42% (n=32) had localized disease, 31% (n=24) had regional disease extension (without nodal involvement) and 27% had regional-nodal (n=2) or distant (n=19) metastases. Cancer-directed surgery was performed in 85%; radiation was performed in 16%. The 1-year, 5-year and median OS were 87%, 49% and 4.6 years respectively. The 1-year, 5-year and median CSS were 89%, 61% and 5.7 years respectively. Less advanced stage and undergoing cancer-directed surgery were favorable prognostic factors. For localized, regional and distant stage the median OS was: not reached at 6.3 years, 4.4 years and 2.0 years respectively (P=0.021); the median CSS was not reached at 6.3 years, 5.0 years and 2.4 years (P=0.068). For patients undergoing versus not undergoing surgery, the median OS was 4.9 vs 0.9 years (P=0.053) and median CSS was 5.7 vs 0.9 years (P=0.011). Tumor size was not significant.
Conclusions: From a population-based analysis of patients with thoracic malignant solitary fibrous tumors, stage and cancer-directed surgery had the greatest impact on OS and CSS. While being amenable to surgery likely reflects more indolent disease and/or better performance status and cardiopulmonary function, the significantly favorable impact of surgery also likely reflects a therapeutic benefit.
Key words
malignant solitary fibrous tumor, lung, pleural, population-based
J Thorac Dis 2011;3:99-104. DOI: 10.3978/j.issn.2072-1439.2011.01.04
|
|
Introduction
Solitary fibrous tumors are rare primary malignancies arising from the submesothelial mesenchymal layer, mostly pleural in origin, though they can arise from extrapleual sites as well (1,2). These tumors often grow to a large size (3,4). Ten to 20% are classified as malignant, which are pathologically characterized by mitoses, necrosis, atypia and hypercellularity (5). Compared to benign solitary fibrous tumors, malignant tumors are characterized radiographically by larger size (6,7), and greater likelihood of PET positivity (6,7), and are characterized clinically by a greater likelihood of symptomatic presentation (6,8,9), more aggressive behavior, greater propensity to recur and/or metastasize, and poorer survival (1,5,6,8-10).
The present study offers a descriptive, retrospective analysis of patients with thoracic malignant solitary fibrous tumors, registered in the population-based Surveillance, Epidemiology, and End Results (SEER) database. This study was undertaken with the goal of better characterizing the overall survival (OS) and cause specific survival (CSS) of thoracic malignant solitary fibrous tumors and the risk factors affecting survival outcomes. This appears to be the first paper to analyze survival outcomes of patients registered in the SEER database with a diagnosis of malignant solitary fibrous tumors, and represents the largest series of these patients.
|
|
Methods
Patient database
The SEER Program collects information from population-based cancer registries throughout the United States. Serial registry data are de-identified and submitted to the United States National Cancer Institute on a biannual basis.
Patients were selected with the SEER Stat case listing session
using the following criteria from the SEER database fields:
“Site recode” = “pleura”, “trachea or mediastinum” or “lung and
bronchus”; and ICD-O-3 Hist/Behav=”solitary fibrous tumor,
malignant.” Only patients actively followed were included (i.e.
autopsy and death certificate only cases were excluded).
The “SEER historic stage A” and “summary stage 2000”
variables of localized, regional (direct extension and/or nodal
involvement) and distant (distant nodal sites and/or distant
metastases) were used to stage patients. The SEER database also
records whether or not a patient has undergone cancer-directed
surgery, which the SEER program considers as any curative or
palliative surgery that removes cancer, excluding biopsies which
remove only a fragment or portion of tumor.
Statistical analysis
Stata version 9.2 (StataCorp, College Station, TX) was used
for data analysis. Actuarial OS was calculated using the Kaplan-
Meier method. For univariate analyses comparing OS between
subgroups, the log-rank test was used. For multivariate analyses
(MVA) assessing the significance and hazard ratios (HR) of
prognostic variables, Cox proportional hazards models were
used. P values
|
|
Results
Patient and tumor characteristics
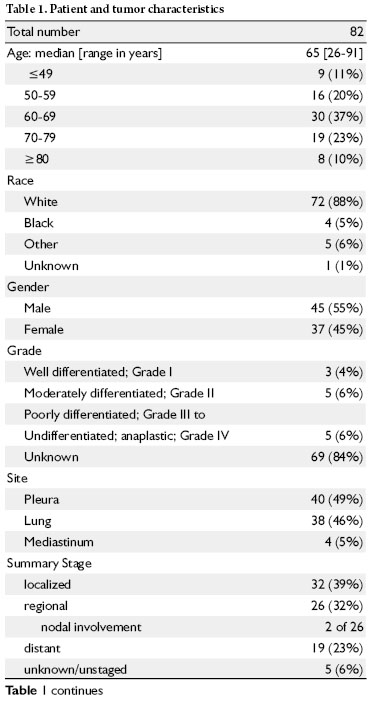
Table 1 summarizes the patient and tumor characteristics of the
study patients. All patients had pathologic diagnosis of malignant
solitary fibrous tumor. The median age at the time of diagnosis
was 65 years. Fifty five percent are males. Of those with available
staging information, 21 of 77 (27%) had nodal or distant
metastases. Of the 56 without nodal or distant metastases, 32
(57%) were classified as “localized” stage disease. Tumor grade
was not available in 84% of patients. Because only 2 patients had
regional nodal disease, they are grouped with the regional via
direct extension patients in the analyses below (regional stage
group).
Among all patients, the follow-up ranged from 1 month – 6.8
years (median 2.2 years). Among patients alive at last follow-up,
the median follow-up was 2.3 years.
Patient treatments
Cancer-directed surgery was performed in 85% of patients,
radiation was performed in 16%, and both radiation and surgery
were performed in 13%. Close to half (47%) of the patients
underwent a radical-extent surgery (see Table 1 footnote).
Among patients with localized, regional and distant disease,97%, 92% and 68%, respectively, underwent cancer-directed
surgery (P=0.019), and among those patients undergoing
surgery, 59%, 48% and 33% (respectively) underwent radical
resection (P=0.53).
Among patients with lung and pleural primary sites, 79% and
90%, respectively, underwent cancer-directed surgery (P=0.18),
and among those patients undergoing surgery, 57% and 44%
(respectively) underwent radical resection (P=0.31)
Patient survival
The 1-year, 2-year and 5-year OS (Fig 1) of patients were 87%,
78% and 49% respectively. Median OS was 4.6 years. The 1-year,
2-year and 5-year CSS (Fig 1) of patients were 89%, 81% and
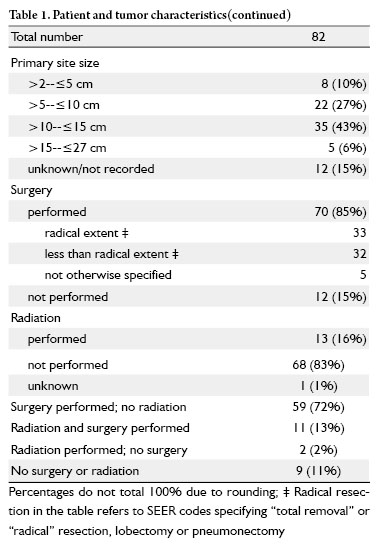
61% respectively. Median CSS was 5.7 years. Table 2 outlines
the univariate analyses of variables potentially impacting OS and
CSS. Significant and borderline significant (P
For localized, regional and distant stage the median OS
(Fig 2a) was: not reached at 6.3 years, 4.4 years and 2.0
years respectively (P=0.021); the median CSS (Fig 2b) was
not reached at 6.3 years, 5.0 years and 2.4 years respectively
(P=0.068). For patients undergoing versus not undergoing
surgery, the median OS (Fig 3a) was 4.9 vs 0.9 years
(P=0.053), and the median CSS (Fig Fig 3b) was 5.7 vs 0.9 years
(P=0.011). While the OS and CSS of those patients treated
without cancer-directed surgery plateaus (i.e. no deaths) beyond
1-year, only 3 patients are at risk beyond 1 year, and thus the
calculated survival beyond 1-year reflects that of only a few
patients.
Table 3 shows the Cox regression analyses, for which cancerdirected
surgery and stage were significant for OS and CSS.
Adding tumor size to the models did not appreciably impact the
HRs or P values of stage and surgical resection, and tumor size
remained not significant.
|
|
Discussion
From the present analyses of patients with malignant solitary
fibrous tumors of the thorax, cancer stage and cancer-directed
surgery of the primary site significantly impact OS and CSS.
From Cox regression analyses, increments in stage were
associated with a HR of ~1.8 for OS and CSS. Cancer-directed
surgery was associated with a HR of 0.3 (>3-fold reduction in
deaths) for OS and 0.2 (5-fold reduction in deaths) for CSS.
While the actuarial OS and CSS of patients undergoing cancerdirected
surgery is similar to those not undergoing surgery
beyond 5-6 years (Fig 3), the small number of patients evaluable
at these time points (particularly those not undergoing surgery)
precludes any definitive conclusions about these findings. Certainly, select patients whose tumors are not resected can
experience a prolonged survival.
Malignant solitary fibrous tumors are generally larger than
benign tumors (6-12), significantly so in some studies (8,10),
though very large tumors can be benign. Perhaps larger tumors
are more likely to have undergone genetic changes (13). While
tumor size has been shown to be prognostic in retrospective
series of patients with benign and malignant solitary fibrous tumors (5,10,11), this study which included only patients with
malignant tumors, and others, including benign and malignant
histologies (6,14), did not demonstrate an effect of size on
survival outcomes.
The survival outcomes reported here are similar to that
reported in a Mayo Clinic study (median survival of 4.6 years,
and 5-year OS of 46%) which included 11 patients with
malignant solitary fibrous tumors (8). In a study of 15 patients with malignant solitary fibrous tumors from Memorial Sloan
Kettering, the 5-year survival was reported to be 55% (10).
A Korean study including 13 patients with malignant solitary
fibrous tumors reported a median survival of 2.0 years (9).
A French study reported a 5 and 10-year survival rate of 89%
among 22 patients with malignant solitary fibrous tumors (of
which only one did not undergo a complete resection) (15).
The observed OS and CSS benefit of cancer-directed surgery
for malignant solitary fibrous tumors in this study likely reflects
a combination of selection of patients who can tolerate surgery,
more indolent disease being amenable to surgical resection
and a therapeutic benefit from surgery. The Cox analyses which
incorporate stage account for the extent of tumor (albeit with a
spectrum of disease extent included within each stage group),
and thus there is a possible therapeutic benefit of surgery. Other
factors used to select patients for surgery, such as performance
status, pulmonary function, cardiac function and comorbid
conditions were not accounted for in these analyses, and also
likely contribute to the survival benefit of surgery. Because of
the retrospective nature of this study, it is not appropriately
designed to address how extent of resection impacts outcome,
though this data suggests that radical resection results in a trend
towards better CSS versus less radical resections. Univariate
analyses in this study suggest that undergoing radiation does not
significantly impact survival outcomes, although, as described
above for surgery, understanding the effect of radiation is
complicated by the retrospective nature of this study. Clinical
responses to radiation have been reported in the literature for
benign (16), and malignant solitary fibrous tumors (17). The
role of adjuvant radiation for solitary fibrous tumors is not
known, though it has been suggested that malignant tumors can
benefit from adjuvant radiotherapy (3,9).
Other weaknesses of the present study include the inability to
ascertain progression/recurrence free survival and to account for
other potentially relevant variables, such as performance status
and tumor grade (which is reported in only 16% of patients,
despite all having pathologic diagnosis). It must be acknowledged
that there are complexities and uncertainties in the pathologic
diagnosis of solitary fibrous tumors, which therefore limits the
interpretation of retrospective analyses such as this study. It is
possible that a pleura mesothelioma or, alternatively, a benign
solitary fibrous tumors was misdiagnosed as malignant solitary
fibrous tumors. The tumor pathology cannot be systematically
reviewed, using modern immunohistochemistry techniques,
to verify and specify the pathologic diagnosis. Likewise,
radiographic imaging is not available to review, which can also
assist in the diagnosis by either CT (18) or PET criteria (6,7).
The strengths of the study include the relatively large number
of patients analyzed, from an unbiased population-based registry.
Analyzing 82 patients allowed investigation of demographic,
clinicopathologic and treatment-related variables. Nevertheless, the number of patients (and number of events) is too small to
analyze outcomes grouped by stage.

Fig 1 Kaplan-Meier overall survival (lower, blue curve) and cause
specific survival (upper, red curve), among all 82 patients.

Fig 2 Kaplan-Meier overall survival (2a) and cause specific survival (2b), grouped by stage.

Fig 3 Kaplan-Meier overall survival (3a) and cause specific survival (3b), grouped by cancer-directed surgery. Those patients undergoing cancer
directed surgery have the higher survival (at

|
|
Conclusions
From a hypothesis generating, retrospective, population-based
registry analysis of patients with thoracic malignant solitary
fibrous tumors, cancer stage and cancer-directed surgery
appear to have the greatest impact on OS and CSS. While being
amenable to surgery likely reflects more indolent disease and/
or better performance status and cardiopulmonary function, the
significantly favorable impact of surgery, when accounting for
tumor size and stage may reflect a therapeutic benefit.
|
|
References
Cite this article as: Milano MT, Singh DP, Zhang H. Thoracic malignant solitary fibrous tumors: A population-based study of survival. J Thorac Dis 2011;3(2):99-104. doi: 10.3978/j.issn.2072-1439.2011.01.04
|

